4.1 Sleeping and Dreaming Revitalize Us for Action
Learning Objectives
- Draw a graphic showing the usual phases of sleep during a normal night, and notate the characteristics of each phase.
- Review the disorders that affect sleep and the costs of sleep deprivation.
- Outline and explain the similarities and differences among the different theories of dreaming.
The lives of all organisms, including humans, are influenced by regularly occurring cycles of behaviours known as biological rhythms. One important biological rhythm is the annual cycle that guides the migration of birds and the hibernation of bears. Women also experience a 28-day cycle that guides their fertility and menstruation. Perhaps the strongest and most important biorhythm is the daily circadian rhythm — from the Latin circa, meaning “about” or “approximately,” and dian, meaning “daily” — that guides the daily waking and sleeping cycle in many animals. Many biological rhythms are coordinated by changes in the level and duration of ambient light, such as when winter turns into summer and when night turns into day. In some animals, such as birds, the pineal gland in the brain is directly sensitive to light, and its activation influences behaviour, such as mating and annual migrations. Light also has a profound effect on humans. We are more likely to experience depression during the dark winter months than during the lighter summer months, an experience known as seasonal affective disorder (SAD), and exposure to bright lights can help reduce this depression (Mayo Clinic Staff, 2007).
Sleep is also influenced by ambient light. The ganglion cells in the retina send signals to a brain area above the thalamus called the suprachiasmatic nucleus, which is the body’s primary circadian pacemaker. The suprachiasmatic nucleus analyzes the strength and duration of the light stimulus and sends signals to the pineal gland when the ambient light level is low or its duration is short. In response, the pineal gland secretes melatonin, a powerful hormone that facilitates the onset of sleep.
Research Focus
Later start times recommended for Canadian schools
McGill University researchers Genevieve Gariépy, Ian Janssen, Mariane Sentenac, and Frank Elgar (2017) investigated the association between sleep and academic performance in Canadian students in Grades 6 to 10. Their research was based on previous findings showing that a significant number of adolescents do not get the recommended amount of sleep. Insufficient sleep is associated with a host of problems, including poor memory, reduced physical and mental health, and a greater number of car accidents.
One of the instigators of insufficient sleep is school start time. Early start times tend to disrupt the sleep of adolescents, whose circadian rhythms undergo a shift in puberty. The researchers analyzed data from over 30,000 students who participated in the 2013/14 Canadian Health Behaviour in School‐Aged Children (HBSC) survey. They found that one-third of students were not getting enough sleep (i.e., between eight and 11 hours per night, depending on the age of the child). While about two-thirds of students were getting the advisable minimum amount of sleep, 60% reported feeling tired when they went to school. They also found that on weekends, students went to bed later, slept for longer, and got up later than on weekdays.
The researchers found that students whose school start time was later got more sleep, were more likely to get the recommended amount of sleep, and were less likely to feel tired in the morning. Their analysis suggests that later start times — for instance, 9:30 a.m. instead of the more typical 8:30 a.m. start time — might help students avoid the problems associated with poor or insufficient sleep. Further research is needed to determine if there are age-specific effects, and experimental research is needed to clarify the causal effects of changing school start times on student sleep and learning.
Sleep stages: Moving through the night
Although we lose consciousness as we sleep, the brain nevertheless remains active. The patterns of sleep have been tracked in thousands of research participants who have spent nights sleeping in research labs (see Figure 4.2) while their brainwaves were recorded by monitors, such as an electroencephalogram (EEG).

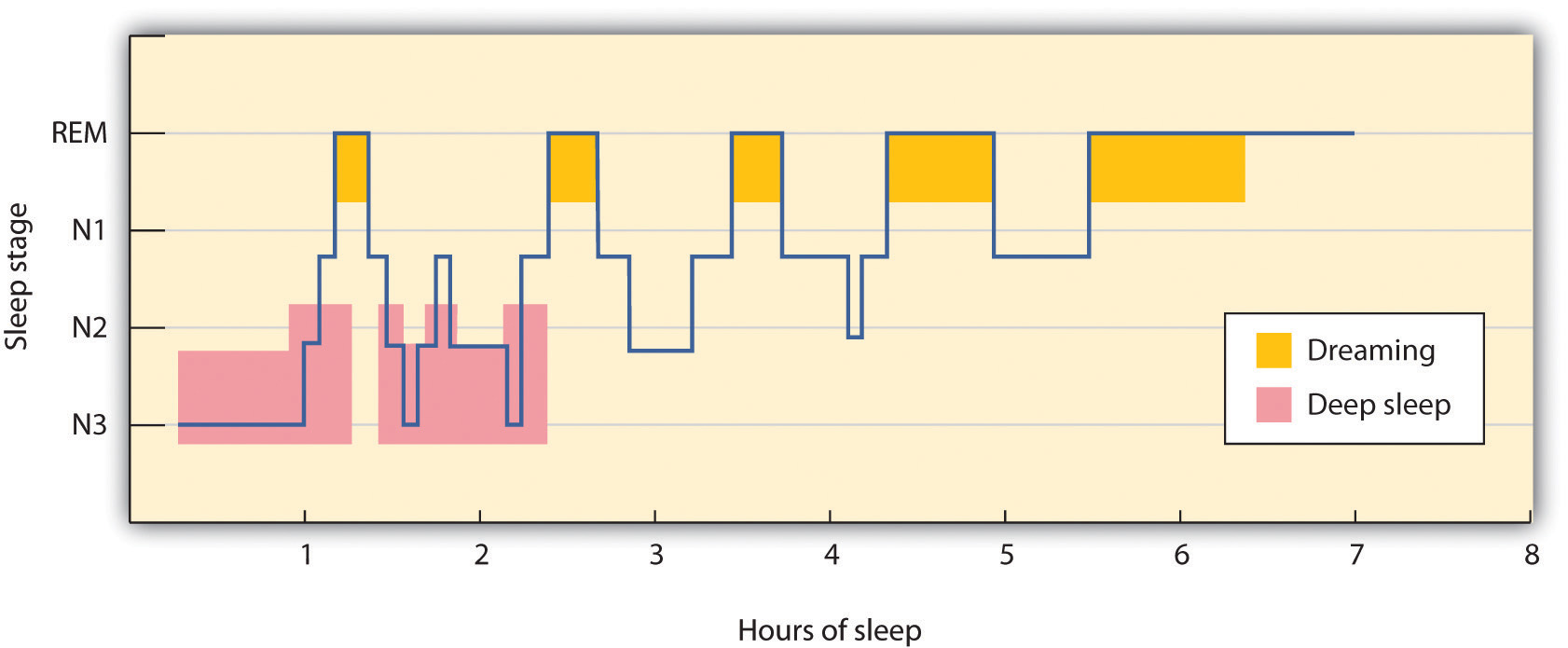
Sleep researchers have found that sleeping people undergo a fairly consistent pattern of sleep stages, each lasting about 90 minutes (see Figure 4.3). These stages are of two major types: rapid eye movement and non-rapid eye movement. Rapid eye movement (REM) sleep is a sleep stage characterized by the presence of quick eye movements and dreaming. REM sleep accounts for about 25% of our total sleep time. During REM sleep, our awareness of external events is dramatically reduced, and consciousness is dominated primarily by internally generated images and a lack of overt thinking (Hobson, 2004). During this sleep stage, our muscles shut down, and this is probably a good thing as it protects us from hurting ourselves or trying to act out the scenes that are playing in our dreams. In contrast, non-rapid eye movement (non-REM) sleep is a deep sleep, characterized by very slow brainwaves, that is further subdivided into three stages: N1, N2, and N3. Each of the sleep stages has its own distinct pattern of brain activity (Dement & Kleitman, 1957).
The brainwaves that are recorded by an EEG as we sleep show that the brain’s activity changes during each stage of sleeping (see Figure 4.4). When we are awake, our brain activity is characterized by the presence of very fast beta waves. When we first begin to fall asleep, the waves get longer, becoming alpha waves, and as we move into stage N1 sleep, which is characterized by the experience of drowsiness, the brain begins to produce even slower theta waves. During stage N1 sleep, some muscle tone is lost as well as most awareness of the environment. Some people may experience sudden jerks or twitches and even vivid hallucinations during this initial stage of sleep.
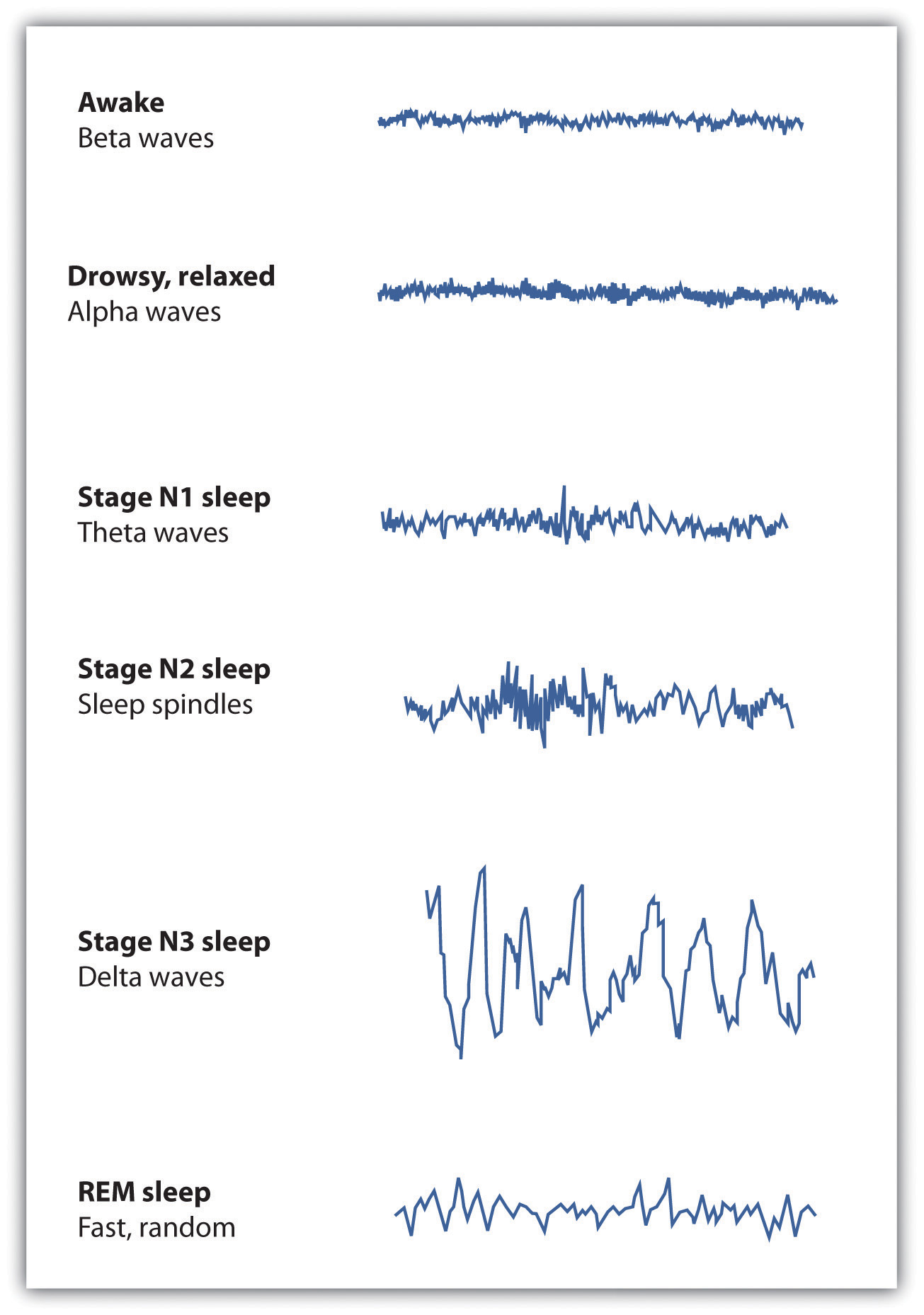
Normally, if we are allowed to keep sleeping, we will move from stage N1 to stage N2 sleep. During stage N2, muscular activity is further decreased, and conscious awareness of the environment is lost. This stage typically represents about half of the total sleep time in normal adults. Stage N2 sleep is characterized by theta waves interspersed with bursts of rapid brain activity known as sleep spindles.
Stage N3, also known as slow wave sleep, is the deepest level of sleep, characterized by an increased proportion of very slow delta waves. This is the stage in which most sleep abnormalities occur, such as sleepwalking, sleeptalking, nightmares, and bedwetting. The sleepwalking murders committed by Mr. Parks would have occurred in this stage. Some skeletal muscle tone remains, making it possible for affected individuals to rise from their beds and engage in sometimes very complex behaviours, but consciousness is distant. Even in the deepest sleep, however, we are still aware of the external world. If smoke enters the room or if we hear the cry of a baby, we are likely to react even though we are sound asleep. These occurrences again demonstrate the extent to which we process information outside consciousness.
After falling initially into a very deep sleep, the brain begins to become more active again, and we normally move into the first period of REM sleep about 90 minutes after falling asleep. REM sleep is accompanied by an increase in heart rate, facial twitches, and the repeated rapid eye movements that give this stage its name. People who are awakened during REM sleep almost always report that they were dreaming, while those awakened in other stages of sleep report dreams much less often. REM sleep is also emotional sleep. Activity in the limbic system, including the amygdala, is increased during REM sleep, and the genitals become aroused, even if the content of the dreams we are having is not sexual. A typical 25-year-old man may have an erection nearly half the night, and the common “morning erection” is left over from the last REM period before waking.
Normally, we will go through several cycles of REM and non-REM sleep each night (see Figure 4.4). We cycle up and down through the stages of sleep. The length of the REM portion of the cycle tends to increase through the night, from about 5 to 10 minutes early in the night to 15 to 20 minutes shortly before awakening in the morning. Dreams also tend to become more elaborate and vivid as the night goes on. Eventually, as the sleep cycle finishes, the brain resumes its faster alpha and beta waves, and we wake up feeling refreshed.
Sleep disorders: Problems in sleeping
According to Statistics Canada (2011), three in five Canadian adults say they feel tired most of the time. These people are suffering from a sleep disorder known as insomnia, defined as persistent difficulty falling or staying asleep. Most cases of insomnia are temporary, lasting from a few days to several weeks, but in some cases, insomnia can last for years.
Insomnia can result from physical disorders, such as pain due to injury or illness, or from psychological problems, such as stress, financial worries, or relationship difficulties. Changes in sleep patterns, such as jet lag, changes in work shift, or even the movement to or from daylight saving time, can produce insomnia. Sometimes the sleep that the insomniac does get is disturbed and nonrestorative, and the lack of quality sleep produces impairment of functioning during the day. Ironically, the problem may be compounded by people’s anxiety over insomnia itself: their fear of being unable to sleep may wind up keeping them awake. Some people may also develop a conditioned anxiety to the bedroom or the bed, but we will return to the concept of conditioning in Chapter 6.
Modern life has introduced a sleep-interference device in the form of technology. The blue light emitted by mobile phones and tablets promotes wakefulness and delays our circadian rhythm by suppressing the release of melatonin, which is a sleep-promoting hormone released near bedtime and during the night. The activities we engage in on our mobile devices have the added effect of mental effort and distraction; instead of calming down, relaxing, and becoming less alert at bedtime, many of us are chatting, watching movies, and engaging in other online activity.
People who have difficulty sleeping may turn to drugs to help them sleep. Barbiturates, benzodiazepines, and other sedatives (see Figure 4.5) are frequently marketed and prescribed as sleep aids, but they may interrupt the natural stages of the sleep cycle, and in the end are likely to do more harm than good. In some cases, they may also promote dependence. Most practitioners of sleep medicine today recommend making environmental and scheduling changes first, followed by therapy for underlying problems, with pharmacological remedies used only as a last resort.

According to the Canadian Sleep Society (Morin, n.d.), there are many steps that can be used to combat insomnia. These are summarized in the table below.
| Behaviour |
Purpose or Effect |
| Learn to relax | Relaxation is helpful when stress or anxiety is part of an insomnia problem. Some relaxation exercises are designed to reduce physical tension, whereas others seek to eliminate intrusive thoughts and worries at bedtime. |
| Give yourself at least one hour to unwind before bedtime | Use this transitional period to read, watch television, listen to music, or simply relax. Do not ruminate about events of the day. Rather, write down your worries, and set aside another time to manage them. |
| Restrict the amount of time you spend in bed to the actual sleep time | People with insomnia often spend excessive amounts of time in bed in an attempt to get enough sleep. Spending too much time in bed may actually lead to poorer sleep quality. |
| Go to bed only when sleepy | Individuals with insomnia often go to bed too early. Such practice is counterproductive because the bed becomes a cue associated with wakefulness rather than with sleep. Postpone your bedtime until you are sleepy. |
| Get out of bed if you can’t sleep | Whenever you are awake for more than 15-20 minutes in bed, get up, go to another room, and engage in some quiet activity. Return to bed only when you feel that sleep is imminent. |
| Arise at the same time every morning | Set the alarm clock, and get out of bed at the same time on weekdays as well as weekends, regardless of the amount of sleep obtained on the previous night. Sticking to a schedule will help regulate your internal biological clock and synchronize your sleep/wake rhythm. |
| Reserve your bed and bedroom for sleep only | Do not read, watch television, or use cell phones or other electronic devices in bed. When you engage in these practices, the bedroom becomes associated with wakefulness rather than with sleepiness. |
| Avoid daytime napping | Among insomnia sufferers, napping is generally counterproductive. A nap disrupts the natural sleep/wake rhythm and interferes with nighttime sleep. |
| Maintain good sleep hygiene | Avoid stimulants (e.g., caffeine) several hours before bedtime. Do not drink alcohol too close to bedtime as it can lead to poor quality sleep. Regular exercise in the late afternoon or early evening may deepen sleep. Keep the bedroom environment quiet, dark, and comfortable. |
Another common sleep problem is sleep apnea, which is a sleep disorder characterized by pauses in breathing that last at least 10 seconds during sleep (Morgenthaler, Kagramanov, Hanak, & Decker, 2006). In addition to preventing restorative sleep, sleep apnea can also cause high blood pressure and may increase the risk of stroke and heart attack (Yaggi et al., 2005).
Most sleep apnea is caused by an obstruction of the walls of the throat that occurs when we fall asleep. It is most common in obese or older individuals who have lost muscle tone and is particularly common in men. Sleep apnea caused by obstructions is usually treated with an air machine that uses a mask to create a continuous pressure that prevents the airway from collapsing, or it may be treated with mouthpieces that keep the airway open. If all other treatments have failed, sleep apnea may be treated with surgery to open the airway.
Narcolepsy is a disorder characterized by extreme daytime sleepiness with frequent episodes of nodding off. The syndrome may also be accompanied by attacks of cataplexy, in which the individual loses muscle tone, resulting in a partial or complete collapse. It is estimated that one in 2,000 people suffer from narcolepsy.
Narcolepsy is, in part, the result of genetics — since people who suffer from the disease lack neurotransmitters that are important in keeping us alert (Taheri, Zeitzer, & Mignot, 2002) — and is also the result of a lack of deep sleep. While most people descend through the sequence of sleep stages before moving back up to REM sleep, narcolepsy sufferers move directly into REM sleep and undergo numerous awakenings during the night, often preventing them from getting a quality sleep.
Narcolepsy can be treated with stimulants, such as amphetamines, to counteract the daytime sleepiness or with antidepressants to treat a presumed underlying depression. However, since these drugs further disrupt already abnormal sleep cycles, these approaches may, in the long run, make the problem worse. Many sufferers find relief by taking a number of planned short naps during the day, and some individuals may find it easier to work in jobs that allow them to sleep during the day and work at night.
Other sleep disorders occur when cognitive or motor processes that should be turned off or reduced in magnitude during sleep operate at levels higher than normal (Mahowald & Schenck, 2000). One example is somnambulism (i.e., sleepwalking), in which the person leaves the bed and moves around while still asleep. Sleepwalking is more common in childhood, with the most frequent occurrences around the age of 12 years. About 4% of adults experience somnambulism (Mahowald & Schenck, 2000).
Sleep terrors is a disruptive sleep disorder, most frequently experienced in childhood, that may involve loud screams and intense panic. The sufferer cannot wake from sleep even though they are trying to. In extreme cases, sleep terrors may result in bodily harm or property damage as the sufferer moves about abruptly. Up to 3% of adults suffer from sleep terrors, which typically occur in sleep stage N3 (Mahowald & Schenck, 2000).
Other sleep disorders include bruxism, in which the sufferer grinds their teeth during sleep; restless legs syndrome, in which the sufferer reports an itching, burning, or otherwise uncomfortable feeling in their legs, usually exacerbated when resting or asleep; and periodic limb movement disorder, in which the sufferer has sudden, involuntary movement of limbs. The last of these, periodic limb movement disorder, can cause sleep disruption and injury for both the sufferer and bed partner.
Although many sleep disorders occur during non-REM sleep, some occur during REM sleep. REM sleep behaviour disorder (Mahowald & Schenck, 2005) is a condition in which people, usually middle-aged or older men, engage in vigorous and bizarre physical activities during REM sleep in response to intense, violent dreams. As their actions may injure themselves or their sleeping partners, this disorder, thought to be neurological in nature, is normally treated with hypnosis and medications.
The heavy costs of not sleeping
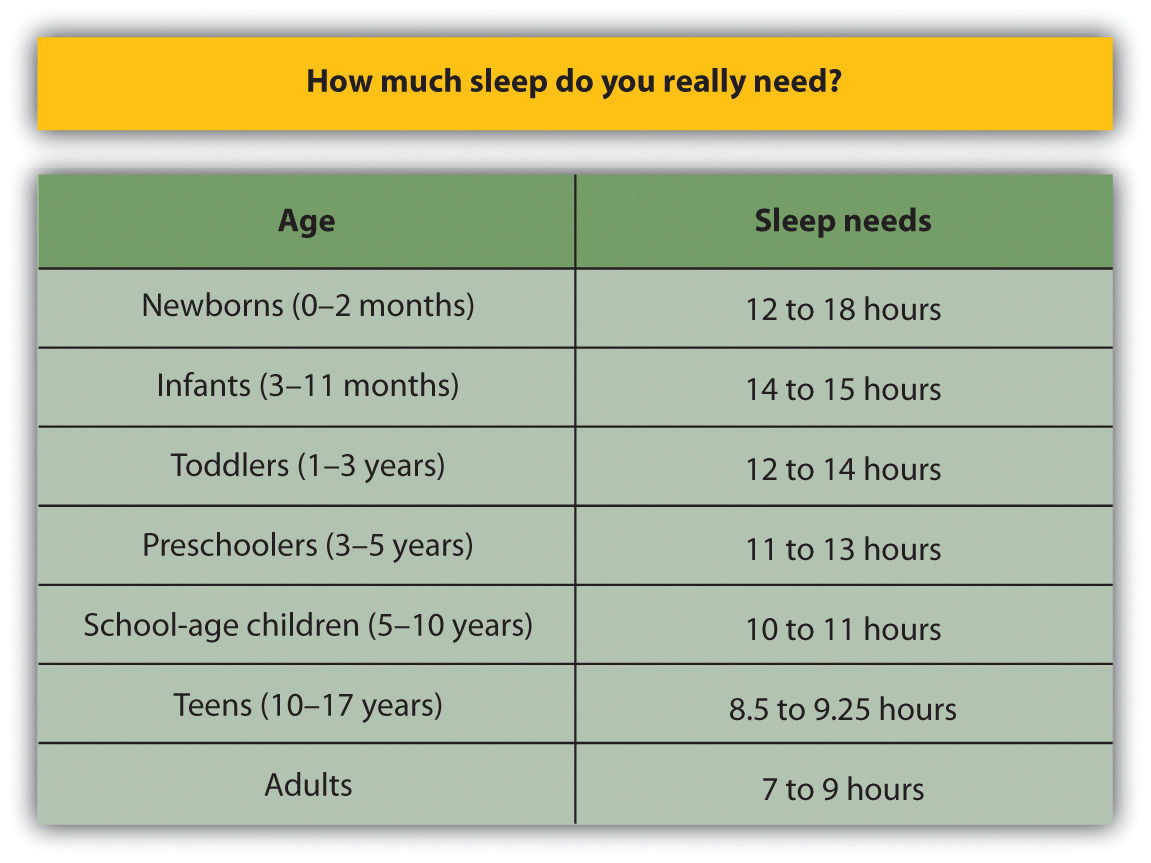
Our preferred sleep times and our sleep requirements vary throughout our life cycle. Newborns tend to sleep between 16 and 18 hours per day, preschoolers tend to sleep between 10 and 12 hours per day, school-aged children and teenagers usually prefer at least nine hours of sleep per night, and most adults say that they require seven to eight hours per night (Mercer, Merritt, & Cowell, 1998; Statistics Canada, 2011). There are also individual differences in need for sleep. Some adults do quite well with fewer than six hours of sleep per night, whereas others need nine hours or more. Mental Health Canada (2014) suggests that adults should get between seven and nine hours of sleep per night (see Figure 4.6), and yet 15% of Canadians average fewer than six and a half hours, and 47% of Canadians stated that they cut down on sleep in an attempt to squeeze more time out of the day.
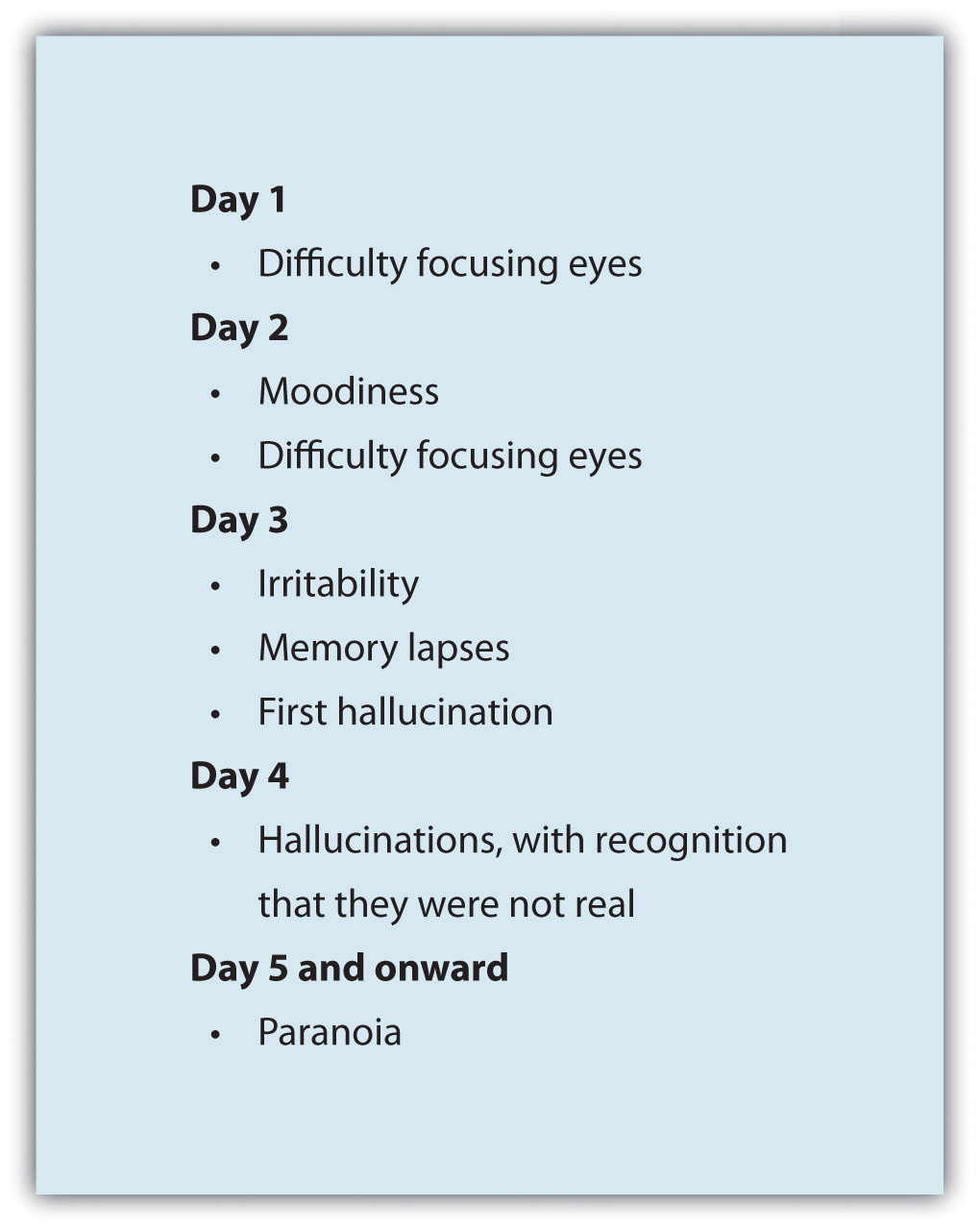
Getting needed rest is difficult, partly because school and work schedules still follow the early-to-rise timetable that was set years ago. We tend to stay up late to enjoy activities in the evening but are then forced to get up early to go to work or school. The situation is particularly bad for university students, who are likely to combine a heavy academic schedule with an active social life and who may, in some cases, also work. Getting enough sleep is a luxury that many of us seem to be unable or unwilling to afford, and yet sleeping is one of the most important things we can do for ourselves. Continued over time, a nightly deficit of even only one or two hours can have a substantial impact on mood and performance (see Figure 4.7).
Sleep has a vital, restorative function. A prolonged lack of sleep results in increased anxiety, diminished performance, and, if severe and extended, even death. Many road accidents involve sleep deprivation, and people who are sleep-deprived show decrements in driving performance similar to those who have ingested alcohol (Hack, Choi, Vijayapalan, Davies, & Stradling, 2001; Williamson & Feyer, 2000). Poor treatment by doctors (Smith-Coggins, Rosekind, Hurd, & Buccino, 1994) and a variety of industrial accidents have also been traced, in part, to the effects of sleep deprivation.
Good sleep is also important to our health and longevity. It is no surprise that we sleep more when we are sick because sleep works to fight infection. Sleep deprivation suppresses immune responses that fight off infection, and it can lead to obesity, hypertension, and memory impairment (Ferrie et al., 2007; Kushida, 2005). Sleeping well can even save our lives. Mary Amanda Dew and colleagues (Dew et al., 2003) found that older adults who had better sleep patterns also lived longer.
Dreams and dreaming
Dreams are the succession of images, thoughts, sounds, and emotions that passes through our minds while sleeping. When people are awakened from REM sleep, they normally report that they have been dreaming, suggesting that people normally dream several times a night; however, most dreams are forgotten on awakening (Dement, 1997). The content of our dreams generally relates to our everyday experiences and concerns as well as our fears and failures (Cartwright, Agargun, Kirkby, & Friedman, 2006; Domhoff, Meyer-Gomes, & Schredl, 2005).
Many cultures regard dreams as having great significance for the dreamer, either by revealing something important about the dreamer’s present circumstances or by predicting the future. The Austrian psychologist Sigmund Freud (1913/1988) analyzed the dreams of his patients to help him understand their unconscious needs and desires, and psychotherapists still make use of this technique today. Freud believed that the primary function of dreams was wish fulfilment, which is the idea that dreaming allows us to act out the desires that we must repress during the day. He differentiated between the manifest content of the dream (i.e., its literal actions) and its latent content (i.e., the hidden psychological meaning of the dream). Freud believed that the real meaning of dreams is often suppressed by the unconscious mind in order to protect the individual from thoughts and feelings that are hard to cope with. By uncovering the real meaning of dreams through psychoanalysis, Freud believed that people could better understand their problems and resolve the issues that create difficulties in their lives.
Although Freud and others have focused on the meaning of dreams, other theories about the causes of dreams are less concerned with their content. One possibility is that we dream primarily to help with memory consolidation, moving information into long-term memory (Alvarenga et al., 2008; Zhang, 2004). Géraldine Rauchs, Béatrice Desgranges, Jean Foret, and Francis Eustache (2005) found that rats that had been deprived of REM sleep after learning a new task were less able to perform the task again later than were rats that had been allowed to dream, and these differences were greater on tasks that involved learning unusual information or developing new behaviours. Jessica Payne and Lynn Nadel (2004) argued that the content of dreams is the result of consolidation; we dream about the things that are being moved into long-term memory. Thus, dreaming may be an important part of the learning that we do while sleeping (Hobson, Pace-Schott, and Stickgold, 2000).
The activation-synthesis theory of dreaming (Hobson & McCarley, 1977; Hobson, 2004) proposes that dreams are our brain’s interpretation of the random firing of neurons in the brain stem. According to this approach, the signals from the brain stem are sent to the cortex, just as they are when we are awake, but because the pathways from the cortex to skeletal muscles are disconnected during REM sleep, the cortex does not know how to interpret the bombardment of signals. As a result, the cortex strings the messages together into the coherent stories we experience as dreams.
The threat simulation theory of dreaming (Revonsuo, 2000) posits that there is evolutionary adaptiveness to dreams. According to this view, dreaming provides a social rehearsal for situations in waking life that could be biologically significant. For example, dreams that contain threats, enemies, social anxiety, or other such elements provide a “rehearsal” for the dreamer with the opportunities to use tactics such as avoidance that could be employed in real life.
Although researchers are still trying to determine the exact causes of dreaming and the meaning of the dream content, one thing remains clear: we need to dream. If we are deprived of REM sleep, we quickly become less able to engage in the important tasks of everyday life until we are finally able to dream again.
Key Takeaways
- Consciousness, our subjective awareness of ourselves and our environment, is functional because it allows us to plan activities and monitor our goals.
- Psychologists believe that consciousness is the result of neural activity in the brain.
- Human and animal behaviour is influenced by biological rhythms, including annual, monthly, and circadian rhythms.
- Sleep consists of two major stages: REM and non-REM sleep. Non-REM sleep has three substages: N1, N2, and N3.
- Each sleep stage is marked by a specific pattern of biological responses and brainwaves.
- Sleep is essential for adequate functioning during the day. Sleep disorders, including insomnia, sleep apnea, and narcolepsy, may make it hard for us to sleep well.
- Dreams occur primarily during REM sleep. Some theories of dreaming, such as Freud’s, are based on the content of the dreams. Other theories of dreaming propose that dreaming is related to memory consolidation. The activation-synthesis theory of dreaming is based only on neural activity. The threat-simulation theory of dreaming holds that dreams provide a way for dreamers to rehearse how to deal with biologically significant events in waking life.
Exercises and Critical Thinking
- If you happen to be home alone one night, try this exercise. At nightfall, leave the lights and any other powered equipment off. Does this influence what time you go to sleep as opposed to your normal sleep time?
- Review your own sleep patterns. Are you getting enough sleep? What makes you think so?
- Review some of the dreams that you have had recently. Consider how each of the theories of dreaming we have discussed would explain your dreams.
Image Attributions
Figure 4.2. 140307_Jwl_Sleep-1 by JBLM PAO is used under a CC BY-NC-SA 2.0 license.
Figure 4.3. Used under a CC BY-NC-SA 4.0 license.
Figure 4.4. Used under a CC BY-NC-SA 4.0 license.
Figure 4.5. The Little Blue Painkillers by Stephen Cummings is used under a CC BY 2.0 license.
Figure 4.6. Used under a CC BY-NC-SA 4.0 license.
Figure 4.7. Used under a CC BY-NC-SA 4.0 license.
Long Descriptions
Figure 4.6. Sleep recommendations based on age:
| Age | Sleep Needs |
|---|---|
| Newborns (0 to 2 months) | 12 to 18 hours |
| Infants (3 to 11 months) | 14 to 15 hours |
| Toddlers (1 to 3 years) | 12 to 14 hours |
| Preschoolers (3 to 5 years) | 11 to 13 hours |
| School-age children (5 to 10 years) | 10 to 11 hours |
| Teens (10 to 17 years) | 8.5 to 9.25 hours |
| Adults | 7 to 9 hours |
Figure 4.7. Effects of sleep deprivation on Day 1: difficulty focusing eyes; Day 2: moodiness, difficulty focusing eyes; Day 3: irritability, memory lapses, first hallucination; Day 4: hallucinations, with recognition that they were not real; and Day 5 onward: paranoia.
References
Alvarenga, T. A., Patti, C. L., Andersen, M. L., Silva, R. H., Calzavara, M. B., Lopez, G.B., . . . Tufik, S. (2008). Paradoxical sleep deprivation impairs acquisition, consolidation and retrieval of a discriminative avoidance task in rats. Neurobiology of Learning and Memory, 90, 624–632.
Cartwright, R., Agargun, M., Kirkby, J., & Friedman, J. (2006). Relation of dreams to waking concerns. Psychiatry Research, 141(3), 261–270.
Dement, W. (1997). What all undergraduates should know about how their sleeping lives affect their waking lives. Sleepless at Stanford. Retrieved from http://www.Stanford.edu/~dement/sleepless.html
Dement, W., & Kleitman, N. (1957). Cyclic variations in EEG during sleep. Electroencephalography & Clinical Neurophysiology, 9, 673–690.
Dew, M. A., Hoch, C. C., Buysse, D. J., Monk, T. H., Begley, A. E., Houck, P. R., . . . Reynolds, C. F., III. (2003). Healthy older adults’ sleep predicts all-cause mortality at 4 to 19 years of follow-up. Psychosomatic Medicine, 65(1), 63–73.
Domhoff, G. W., Meyer-Gomes, K., & Schredl, M. (2005). Dreams as the expression of conceptions and concerns: A comparison of German and American college students. Imagination, Cognition and Personality, 25(3), 269–282.
Ferrie, J. E., Shipley, M. J., Cappuccio, F. P., Brunner, E., Miller, M. A., Kumari, M., & Marmot, M. G. (2007). A prospective study of change in sleep duration: Associations with mortality in the Whitehall II cohort. Sleep, 30(12), 1659–1666.
Freud, S. (1913/1988). The interpretation of dreams (Special ed.). Birmingham, AL: The Classics of Medicine Library. (Original work published 1913)
Gariépy, G., Janssen, I., Sentenac, M., & Elgar, F. J. (2017). School start time and sleep in Canadian adolescents. Journal of Sleep Research, 26(2), 195–201.
Hack, M. A., Choi, S. J., Vijayapalan, P., Davies, R. J. O., & Stradling, J. R. S. (2001). Comparison of the effects of sleep deprivation, alcohol and obstructive sleep apnoea (OSA) on simulated steering performance. Respiratory Medicine, 95(7), 594–601.
Hobson, A. (2004). A model for madness? Dream consciousness: Our understanding of the neurobiology of sleep offers insight into abnormalities in the waking brain. Nature, 430, 69–95.
Hobson, J. A., & McCarley, R. (1977). The brain as a dream state generator: An activation-synthesis hypothesis of the dream process. American Journal of Psychiatry, 134, 1335–1348.
Hobson, J. A., Pace-Schott, E. F., & Stickgold, R. (2000). Dreaming and the brain: Toward a cognitive neuroscience of conscious states. Behavioral and Brain Sciences, 23(6), 793–842; 904–1018; 1083–1121.
Kushida, C. (2005). Sleep deprivation: basic science, physiology, and behavior. London, England: Informa Healthcare.
Mahowald, M., & Schenck, C. (2000). REM sleep parasomnias. In M. H. Kryger, T. Roth, & C. Dement (Eds.), Principles and practice of sleep medicine (3rd ed., pp. 724–741). Philadelphia, PA: W. B. Saunders.
Mahowald, M., & Schenck, C. (2005). REM sleep behavior disorder. Handbook of Clinical Neurophysiology, 6, 245–253.
Mayo Clinic Staff. (2007). Seasonal affective disorder (SAD): Treatment and drugs. Mayo Clinic. Retrieved from http://www.mayoclinic.com/health/seasonal-affective-disorder/DS00195/DSECTION=treatments%2Dand%2Ddrugs
Mental Health Canada. (2014). Understanding sleep. Retrieved from http://www.mentalhealthcanada.com/article_detail.asp?lang=e&id=28
Mercer, P., Merritt, S., & Cowell, J. (1998). Differences in reported sleep need among adolescents. Journal of Adolescent Health, 23(5), 259–263.
Morgenthaler, T. I., Kagramanov, V., Hanak, V., & Decker, P. A. (2006). Complex sleep apnea syndrome: Is it a unique clinical syndrome? Sleep, 29(9), 1203–1209.
Morin, C. M. (n.d.). Insomnia: Patient information brochure. Canadian Sleep Society. Retrieved from https://css-scs.ca/resources/brochures/insomnia
National Institute of Neurological Disorders and Stroke. (2008). Brain basics: Understanding sleep. Retrieved from https://www.education.ninds.nih.gov/brochures/Brain-Basics-Sleep-6-10-08-pdf-508.pdf
Payne, J., & Nadel, L. (2004). Sleep, dreams, and memory consolidation: The role of the stress hormone cortisol. Learning & Memory, 11(6), 671–678.
Rauchs, G., Desgranges, B., Foret, J., & Eustache, F. (2005). The relationships between memory systems and sleep stages. Journal of Sleep Research, 14, 123–140.
Revonsuo, A. (2000). The reinterpretation of dreams: An evolutionary hypothesis of the function of dreaming. Behavioral and Brain Sciences, 23(6), 877–901.
Ross, J. J. (1965). Neurological findings after prolonged sleep deprivation. Archives of Neurology, 12, 399–403.
Smith-Coggins, R., Rosekind, M. R., Hurd, S., & Buccino, K. R. (1994). Relationship of day versus night sleep to physician performance and mood. Annals of Emergency Medicine, 24(5), 928–934.
Statistics Canada. (2011). General social survey – 2010: Overview of the time use of Canadians. Retrieved from https://www150.statcan.gc.ca/n1/pub/89-647-x/89-647-x2011001-eng.pdf
Taheri, S., Zeitzer, J. M., & Mignot, E. (2002). The role of hypocretins (Orexins) in sleep regulation and narcolepsy. Annual Review of Neuroscience, 25, 283–313.
Williamson, A., & Feyer, A. (2000). Moderate sleep deprivation produces impairments in cognitive and motor performance equivalent to legally prescribed levels of alcohol intoxication. Occupational and Environmental Medicine, 57(10), 649–655.
Yaggi, H. K., Concato, J., Kernan, W. N., Lichtman, J. H., Brass, L. M., & Mohsenin, V. (2005). Obstructive sleep apnea as a risk factor for stroke and death. The New England Journal of Medicine, 353(19), 2034–2041.
Zhang, J. (2004). Memory process and the function of sleep. Journal of Theoretics, 6(6), 1–7.
