12.3 Understanding Stress
Learning Objectives
- Differentiate between stimulus-based and response-based definitions of stress.
- Define stress as a process.
- Differentiate between good stress and bad stress.
- Describe the early contributions of Hans Selye and Walter Cannon to the stress research field.
- Understand the physiological basis of stress and describe the general adaptation syndrome.
The term stress as it relates to the human condition first emerged in scientific literature in the 1930s, but it did not enter the popular vernacular until the 1970s (Lyon, 2012). Today, we often use the term loosely in describing a variety of unpleasant feeling states; for example, we often say we are stressed out when we feel frustrated, angry, conflicted, overwhelmed, or fatigued. Despite the widespread use of the term, stress is a fairly vague concept that is difficult to define with precision.
Researchers have had a difficult time agreeing on an acceptable definition of stress. Some have conceptualized stress as a demanding or threatening event or situation (e.g., a high-stress job, overcrowding, and long commutes to work). Such conceptualizations are known as stimulus-based definitions because they characterize stress as a stimulus that causes certain reactions. Stimulus-based definitions of stress are problematic, however, because they fail to recognize that people differ in how they view and react to challenging life events and situations. For example, a conscientious student who has studied diligently all semester would likely experience less stress during final exams week than would a less responsible, unprepared student.
Others have conceptualized stress in ways that emphasize the physiological responses that occur when faced with demanding or threatening situations (e.g., increased arousal). These conceptualizations are referred to as response-based definitions because they describe stress as a response to environmental conditions. For example, the endocrinologist Hans Selye, a famous stress researcher, once defined stress as the “response of the body to any demand, whether it is caused by, or results in, pleasant or unpleasant conditions” (Selye, 1976, p. 74). Selye’s definition of stress is response-based in that it conceptualizes stress chiefly in terms of the body’s physiological reaction to any demand that is placed on it. Neither stimulus-based nor response-based definitions provide a complete definition of stress. Many of the physiological reactions that occur when faced with demanding situations (e.g., accelerated heart rate) can also occur in response to things that most people would not consider to be genuinely stressful, such as receiving unanticipated good news like an unexpected promotion or raise.
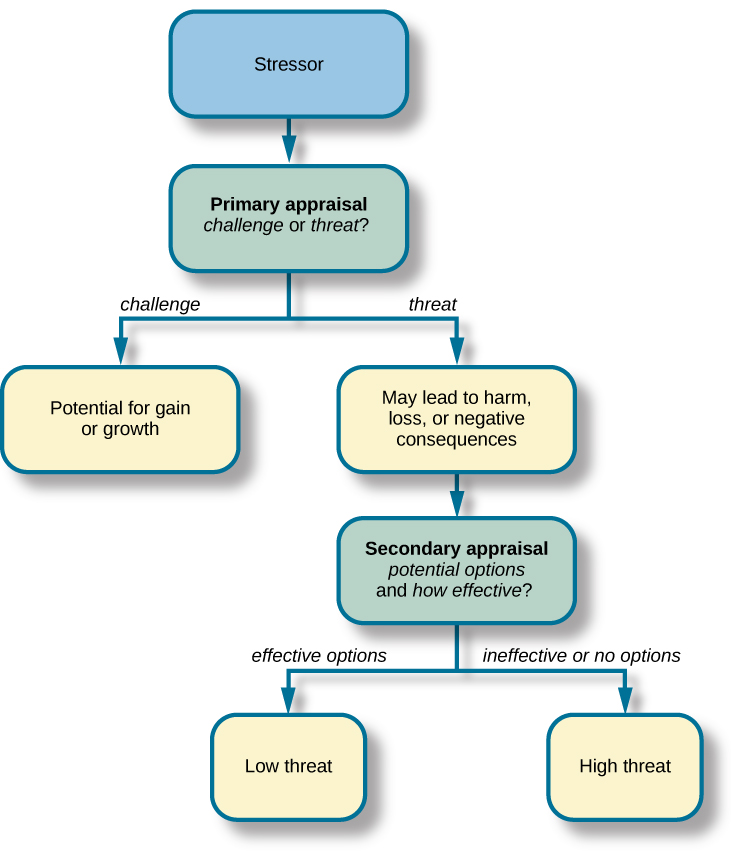
A useful way to conceptualize stress is to view it as a process whereby an individual perceives and responds to events that they appraise as overwhelming or threatening to their wellbeing (Lazarus & Folkman, 1984). A critical element of this definition is that it emphasizes the importance of how we appraise — that is, judge — demanding or threatening events, often referred to as stressors; these appraisals, in turn, influence our reactions to such events. Two kinds of appraisals of a stressor are especially important in this regard: primary and secondary appraisals. A primary appraisal involves judgment about the degree of potential harm or threat to wellbeing that a stressor might entail. A stressor would likely be appraised as a threat if one anticipates that it could lead to some kind of harm, loss, or other negative consequence; conversely, a stressor would likely be appraised as a challenge if one believes that it carries the potential for gain or personal growth. For example, an employee who is promoted to a leadership position would likely perceive the promotion as a much greater threat if they believed the promotion would lead to excessive work demands than if they viewed it as an opportunity to gain new skills and grow professionally. Similarly, a college student on the cusp of graduation may face the change as a threat or a challenge (see Figure 12.11).

The perception of a threat triggers a secondary appraisal (see Figure 12.12), meaning a judgment of the options available to cope with a stressor as well as perceptions of how effective such options will be (Lyon, 2012). As you may recall from what you learned about self-efficacy, an individual’s belief in their ability to complete a task is important (Bandura, 1994). A threat tends to be viewed as less catastrophic if one believes something can be done about it (Lazarus & Folkman, 1984). Imagine that two middle-aged women, Robin and Maria, perform breast self-examinations one morning and each woman notices a lump on the lower region of her left breast. Although both women view the breast lump as a potential threat (i.e., primary appraisal), their secondary appraisals differ considerably. In considering the breast lump, some of the thoughts racing through Robin’s mind are: “Oh my God, I could have breast cancer! What if the cancer has spread to the rest of my body, and I cannot recover? What if I have to go through chemotherapy? I’ve heard that experience is awful! What if I have to quit my job? My husband and I won’t have enough money to pay the mortgage. Oh, this is just horrible. I can’t deal with it!” On the other hand, Maria thinks: “Hmm, this may not be good. Although most times these things turn out to be benign, I need to have it checked out. If it turns out to be breast cancer, there are doctors who can take care of it because the medical technology today is quite advanced. I’ll have a lot of different options, and I’ll be just fine.” Clearly, Robin and Maria have different outlooks on what might turn out to be a very serious situation. Robin seems to think that little could be done about it, whereas Maria believes that, worst case scenario, a number of options that are likely to be effective would be available. As such, Robin would clearly experience greater stress than would Maria.
To be sure, some stressors are inherently more stressful than others in that they are more threatening and leave less potential for variation in cognitive appraisals (e.g., objective threats to one’s health or safety). Nevertheless, appraisal will still play a role in augmenting or diminishing our reactions to such events (Everly & Lating, 2002).
If a person appraises an event as harmful and believes that the demands imposed by the event exceed the available resources to manage or adapt to it, the person will subjectively experience a state of stress. In contrast, if one does not appraise the same event as harmful or threatening, they are unlikely to experience stress. According to this definition, environmental events trigger stress reactions by the way they are interpreted and the meanings they are assigned. In short, stress is largely in the eye of the beholder: it’s not so much what happens to you as it is how you respond (Selye, 1976).
Good stress?
Although stress carries a negative connotation, at times it may be of some benefit. Stress can motivate us to do things in our best interests, such as study for exams, visit the doctor regularly, exercise, and perform to the best of our ability at work. Indeed, Selye (1974) pointed out that not all stress is harmful and that stress can sometimes be a positive, motivating force that can improve the quality of our lives. This kind of stress, which Selye called eustress — from the Greek eu meaning “good” — is a good kind of stress associated with positive feelings, optimal health, and performance. A moderate amount of stress can be beneficial in challenging situations. For example, athletes may be motivated and energized by pregame stress, and students may experience similar beneficial stress before a major exam. Indeed, research shows that moderate stress can enhance both immediate and delayed recall of educational material. Male participants in one study who memorized a scientific text passage showed improved memory of the passage immediately after exposure to a mild stressor as well as one day following exposure to the stressor (Hupbach & Fieman, 2012).
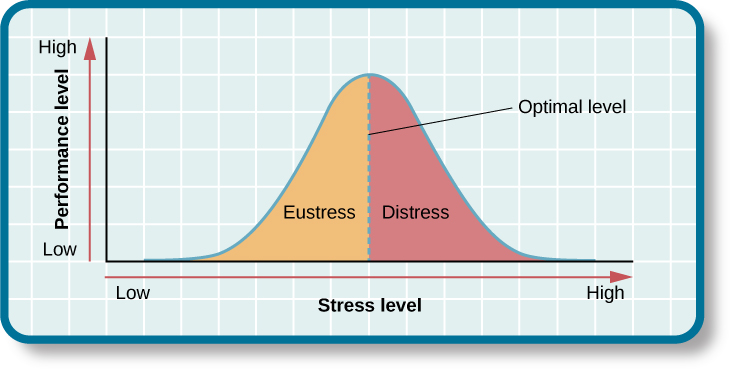
Increasing one’s level of stress will cause performance to change in a predictable way. As stress increases, so do performance and general wellbeing (i.e., eustress); when stress levels reach an optimal level, the highest point of the curve, performance reaches its peak (see Figure 12.13). A person at this stress level is colloquially at the top of their game, meaning they feel fully energized, focused, and can work with minimal effort and maximum efficiency. However, when stress exceeds this optimal level, it is no longer a positive force, and it becomes excessive and debilitating, or what Selye termed distress — from the Latin dis meaning “bad.” People who reach this level of stress feel burned out; they are fatigued, exhausted, and their performance begins to decline. If the stress remains excessive, health may begin to erode as well (Everly & Lating, 2002).
The prevalence of stress
As we mentioned, defining stress is problematic. Understanding the prevalence of stress needs to account both for the stressors and also individual perceptions of those stressors. Statistics Canada regularly asks Canadians about their perceptions of how much stress they experience. The proportion of Canadian adults of working age who report that most days are “quite a bit” or “extremely stressful” is around 25% (Statistics Canada, 2019). Teens and older adults report less stress. Of course, there are many reasons why stress is perceived to be highest by those in the middle of the lifespan. Sources of stress include work, money worries, children, partners, parents, lack of time, responsibilities, and so on.
Stress is an experience that evokes a variety of responses, including those that are physiological (e.g., accelerated heart rate, headaches, or gastrointestinal problems), cognitive (e.g., difficulty concentrating or making decisions), and behavioural (e.g., drinking alcohol, smoking, or taking actions directed at eliminating the cause of the stress). Although stress can be positive at times, it can have deleterious health implications, contributing to the onset and progression of a variety of physical illnesses and diseases (Cohen & Herbert, 1996).
The scientific study of how stress and other psychological factors impact health falls within the realm of health psychology, a subfield of psychology devoted to understanding the importance of psychological influences on health, illness, and how people respond when they become ill (Taylor, 1999). Health psychology emerged as a discipline in the 1970s, a time during which there was increasing awareness of the role behavioural and lifestyle factors play in the development of illnesses and diseases (Straub, 2007). In addition to studying the connection between stress and illness, health psychologists investigate issues such as why people make certain lifestyle choices (e.g., smoking or eating unhealthy food despite knowing the potential adverse health implications of such behaviours). Health psychologists also design and investigate the effectiveness of interventions aimed at changing unhealthy behaviours. Perhaps one of the more fundamental tasks of health psychologists is to identify which groups of people are especially at risk for negative health outcomes, based on psychological or behavioural factors. For example, measuring differences in stress levels among demographic groups and how these levels change over time can help identify populations who may have an increased risk for illness or disease.
Early contributions to the study of stress
As previously stated, scientific interest in stress goes back nearly a century. One of the early pioneers in the study of stress was Walter Cannon (1871–1945), an eminent American physiologist at Harvard Medical School (see Figure 12.14). In the early part of the 20th century, Cannon was the first to identify the body’s physiological reactions to stress. Recall the Cannon-Bard theory of emotion, which stated that emotion is accompanied by physiological arousal. Cannon first articulated and named the fight-or-flight response, which is the nervous system’s sympathetic response to a significant stressor.

Cannon and the fight-or-flight response
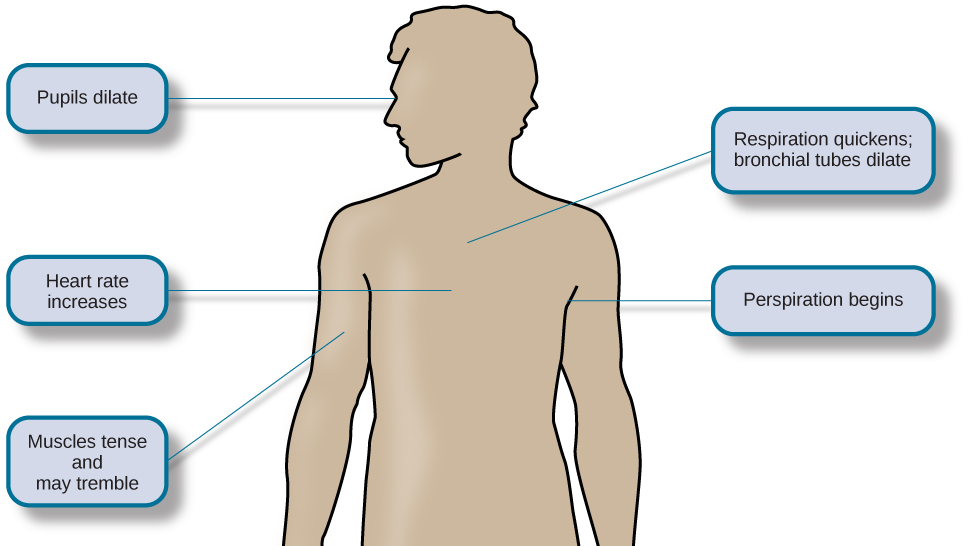
Imagine that you are hiking in the beautiful Rocky Mountains on a warm and sunny spring day. At one point during your hike, a large, frightening-looking black bear appears from behind a stand of trees and sits about 50 metres from you. The bear notices you, sits up, and begins to lumber in your direction. In addition to thinking, “This is definitely not good,” a constellation of physiological reactions begins to take place inside you. Prompted by a deluge of epinephrine (i.e., adrenaline) and norepinephrine (i.e., noradrenaline) from your adrenal glands, your pupils begin to dilate. Your heart starts to pound and speeds up, you begin to breathe heavily and perspire, you get butterflies in your stomach, and your muscles become tense, preparing you to take some kind of direct action. Cannon proposed that this reaction, which he called the fight-or-flight response, occurs when a person experiences very strong emotions — especially those associated with a perceived threat (Cannon, 1932). During the fight-or-flight response, the body is rapidly aroused by activation of both the sympathetic nervous system and the endocrine system (see Figure 12.15). This arousal helps prepare the person to either confront or flee from a perceived threat.
According to Cannon (1932), the fight-or-flight response is a built-in mechanism that assists in maintaining homeostasis, which is an internal environment in which physiological variables such as blood pressure, respiration, digestion, and temperature are stabilized at levels optimal for survival. Thus, Cannon viewed the fight-or-flight response as adaptive because it enables us to adjust internally and externally to changes in our surroundings, which is helpful in survival. Because you do not have to consciously activate your flight-or-fight response, you can rely on its arousal to provide you with the best chance of defeating or running away from a threat like a black bear. Unfortunately, this response also gets triggered when the threat is not real but perceived. We’ll return to this later.
Selye and the general adaptation syndrome
Another important early contributor to the stress field was Hans Selye, mentioned earlier, who would eventually become one of the world’s foremost experts in the study of stress (see Figure 12.16). As a young assistant in the biochemistry department at McGill University in the 1930s, Selye was engaged in research involving sex hormones in rats. Although he was unable to find an answer for what he was initially researching, he incidentally discovered that when exposed to prolonged negative stimulation (i.e., stressors) — such as extreme cold, surgical injury, excessive muscular exercise, and shock — the rats showed signs of adrenal enlargement, thymus and lymph node shrinkage, and stomach ulceration (1936). Selye realized that these responses were triggered by a coordinated series of physiological reactions that unfold over time during continued exposure to a stressor. These physiological reactions were nonspecific, which means that regardless of the type of stressor, the same pattern of reactions would occur. What Selye discovered was the general adaptation syndrome, the body’s nonspecific physiological response to stress.
The general adaptation syndrome (see Figure 12.17) consists of three stages: (1) alarm reaction, (2) stage of resistance, and (3) stage of exhaustion (Selye, 1936; 1976). Alarm reaction describes the body’s immediate reaction upon facing a threatening situation or emergency, and it is roughly analogous to the fight-or-flight response described by Cannon. During an alarm reaction, you are alerted to a stressor, and your body alarms you with a cascade of physiological reactions that provide you with the energy to manage the situation. A person who wakes up in the middle of the night to discover their house is on fire, for example, is experiencing an alarm reaction.

If exposure to a stressor is prolonged, the organism will enter the stage of resistance. During this stage, the initial shock of alarm reaction has worn off and the body has adapted to the stressor. Nevertheless, the body also remains on alert and is prepared to respond as it did during the alarm reaction, although with less intensity. For example, suppose a child who went missing is still missing 72 hours later. Although the parents would obviously remain extremely disturbed, the magnitude of physiological reactions would likely have diminished over the 72 intervening hours due to some adaptation to this event.
If exposure to a stressor continues over a longer period of time, the stage of exhaustion ensues. At this stage, the person is no longer able to adapt to the stressor, and the body’s ability to resist becomes depleted as physical wear takes its toll on the body’s tissues and organs. As a result, illness, disease, and other permanent damage to the body — even death — may occur. If a missing child still remained missing after three months, the long-term stress associated with this situation may cause a parent to literally faint with exhaustion at some point or even to develop a serious and irreversible illness.
In short, Selye’s general adaptation syndrome suggests that stressors tax the body via a three-phase process — an initial jolt, subsequent readjustment, and a later depletion of all physical resources — that ultimately lays the groundwork for serious health problems and even death. It should be pointed out, however, that this model is a response-based conceptualization of stress, focusing exclusively on the body’s physical responses while largely ignoring psychological factors such as appraisal and interpretation of threats. Nevertheless, Selye’s model has had an enormous impact on the field of stress because it offers a general explanation for how stress can lead to physical damage and, thus, disease. As we shall discuss later, prolonged or repeated stress has been implicated in the development of a number of disorders such as hypertension and coronary artery disease.
The physiological basis of stress
What goes on inside our bodies when we experience stress? The physiological mechanisms of stress are extremely complex, but they generally involve the work of two systems—the sympathetic nervous system and the hypothalamic-pituitary-adrenal axis, known as the HPA axis. When a person first perceives something as stressful (i.e., Selye’s alarm reaction), the sympathetic nervous system triggers arousal via the release of adrenaline from the adrenal glands. Release of these hormones activates the fight-or-flight responses to stress (Cannon, 1932), such as accelerated heart rate and respiration. At the same time, the HPA axis, which is primarily endocrine in nature, becomes especially active, although it works much more slowly than the sympathetic nervous system. In response to stress, the hypothalamus, one of the limbic structures in the brain, releases corticotrophin-releasing factor, a hormone that causes the pituitary gland to release adrenocorticotropic hormone (ACTH); the ACTH then activates the adrenal glands to secrete a number of hormones into the bloodstream (see Figure 12.18). An important hormone in this process is cortisol, which can affect virtually every organ within the body. Cortisol is commonly known as a stress hormone and helps provide that boost of energy when we first encounter a stressor, preparing us to run away or fight. However, sustained elevated levels of cortisol weaken the immune system.

In short bursts, this process can have some favorable effects, such as providing extra energy, improving immune system functioning temporarily, and decreasing pain sensitivity. However, extended release of cortisol — as would happen with prolonged or chronic stress — often comes at a high price. High levels of cortisol have been shown to produce a number of harmful effects. For example, increases in cortisol can significantly weaken our immune system (Glaser & Kiecolt-Glaser, 2005), and high levels are frequently observed among depressed individuals (Geoffroy, Hertzman, Li, & Power, 2013). In summary, a stressful event causes a variety of physiological reactions that activate the adrenal glands, which in turn release epinephrine, norepinephrine, and cortisol. These hormones affect a number of bodily processes in ways that prepare the stressed person to take direct action but also in ways that may heighten the potential for illness.
When stress is extreme or chronic, it can have profoundly negative consequences. For example, stress often contributes to the development of certain psychological disorders, including post-traumatic stress disorder, major depressive disorder, and other serious psychiatric conditions. Additionally, we noted earlier that stress is linked to the development and progression of a variety of physical illnesses and diseases. For example, researchers in one study found that people injured during the September 11, 2001, World Trade Center disaster or who developed post-traumatic stress symptoms afterward later suffered significantly elevated rates of heart disease (Jordan, Miller-Archie, Cone, Morabia, & Stellman, 2011). Another investigation yielded that self-reported stress symptoms among aging and retired Finnish food industry workers were associated with morbidity 11 years later. This study also predicted the onset of musculoskeletal, nervous system, and endocrine and metabolic disorders (Salonen, Arola, Nygård, & Huhtala, 2008). Another study reported that male South Korean manufacturing employees who reported high levels of work-related stress were more likely to catch the common cold over the next several months than were those employees who reported lower work-related stress levels (Park et al., 2011). Later, we will explore the mechanisms through which stress can produce physical illness and disease.
Source: Adapted from Spielman et al. (2019).
Key Takeaways
- There are a variety of ways to define stress, but one important component is the perception of being overwhelmed or under threat.
- Our appraisals of stressors influence our reactions to them.
- Primary appraisal involves judging the potential harm or threat to wellbeing of a stressor.
- Secondary appraisal involves judging what options are available to cope with the stressor and the likely effectiveness of them.
- Health psychology encompasses the scientific study of stress, its effects, and how people react to stress.
- One of the body’s responses to stress is the flight-or-fight response. The physiological changes associated with the flight-or-fight response are an adaptation for dealing with a possible threat.
- Hans Selye described the three stages in the general adaptation syndrome as the body’s response to stress: alarm, resistance, and exhaustion. Alarm contains the initial flight-or-fight response.
- The physiological mechanisms of the flight-or-fight response include the sympathetic and parasympathetic nervous systems.
- Extreme or chronic stress heightens the potential for illness due to the prolonged effects of the physiological response to stress.
Image Attributions
Figure 12.11. Used under a CC BY 4.0 license.
Figure 12.12. Used under a CC BY 4.0 license.
Figure 12.13. Used under a CC BY 4.0 license.
Figure 12.14. Walter Bradford Cannon by unknown author is used under a CC BY 4.0 license.
Figure 12.15. Used under a CC BY 4.0 license.
Figure 12.16. Used under a CC BY 4.0 license.
Figure 12.17. Used under a CC BY 4.0 license.
Figure 12.18. Used under a CC BY 4.0 license.
References
Bandura, A. (1994). Self-efficacy. In V. S. Ramachandran (Ed.), Encyclopedia of human behavior (Vol. 4, pp. 71–81). New York, NY: Academic Press.
Cannon, W. B. (1932). The wisdom of the body. New York, NY: W. W. Norton.
Cohen, S., & Herbert, T. B. (1996). Health psychology: Psychological factors and physical disease from the perspective of human psychoneuroimmunology. Annual Review of Psychology, 47, 113–142.
Everly, G. S., & Lating, J. M. (2002). A clinical guide to the treatment of the human stress response (2nd ed.). New York, NY: Kluwer Academic/Plenum Publishing.
Geoffroy, M. C., Hertzman, C., Li, L., & Power, C. (2013). Prospective association of morning salivary cortisol with depressive symptoms in mid-life: A life-course study. PLoS ONE, 8(11), 1–9.
Glaser, R., & Kiecolt-Glaser, J. K. (2005). Stress-induced immune dysfunction: Implications for health. Nature Reviews Immunology, 5, 243–251.
Hupbach, A., & Fieman, R. (2012). Moderate stress enhances immediate and delayed retrieval of educationally relevant material in healthy young men. Behavioral Neuroscience, 126, 819–825.
Jordan, H. T., Miller-Archie, S. A., Cone, J. E., Morabia, A., & Stellman, S. D. (2011). Heart disease among those exposed to the September 11, 2001 World Trade Center disaster: Results from the World Trade Center Health Registry. Preventive Medicine: An International Journal Devoted to Practice and Theory, 53, 370–376.
Lazarus, R. P., & Folkman, S. (1984). Stress, appraisal, and coping. New York, NY: Springer.
Lyon, B. L. (2012). Stress, coping, and health. In V. H. Rice (Ed.), Handbook of stress, coping, and health: Implications for nursing research, theory, and practice (2nd ed., pp. 2–20). Thousand Oaks, CA: Sage.
Park, S. G., Kim, H. C., Min, J. Y., Hwang, S. H., Park, Y. S., & Min, K. B. (2011). A prospective study of work stressors and the common cold. Occupational Medicine, 61, 53–56.
Salonen, P., Arola, H., Nygård, C., & Huhtala, H. (2008). Long-term associations of stress and chronic diseases in ageing and retired employees. Psychology, Health, and Medicine, 13, 55–62.
Selye, H. (1936). A syndrome produced by diverse nocuous agents. Nature, 138, 32–33.
Selye, H. (1974). Stress without distress. Philadelphia, PA: Lippencott.
Selye, H. (1976). The stress of life (Rev. ed.). New York, NY: McGraw-Hill.
Spielman, R., Dumper, K., Jenkins, W., Lacombe, A., Lovett, M., & Perlmutter, M. (2019). Stress, lifestyle, and health. In OpenStax, Psychology. OpenStax CNX. Retrieved from https://cnx.org/contents/Sr8Ev5Og@12.2:oEYbq2uU@9
Statistics Canada. (2019). Perceived life stress, by age group (Table 13-10-0096-04). Retrieved from https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310009604
Straub, R. O. (2007). Health psychology: A biopsychosocial approach (2nd ed.). New York, NY: Worth.
Taylor, S. E. (1999). Health psychology (4th ed.). Boston, MA: McGraw-Hill.

{kind=link}