15.5 Mood Disorders
Learning Objectives
- Summarize and differentiate major depressive disorder and bipolar disorder.
- Explain the genetic and environmental factors that increase the likelihood that a person will develop a mood disorder.
The everyday variations in our feelings of happiness and sadness reflect our mood, which can be defined as the positive or negative feelings that are in the background of our everyday experiences. In most cases, we are in a relatively good mood, and this positive mood has some positive consequences — it encourages us to do what needs to be done and to make the most of the situations we are in (Isen, 2003). When we are in a good mood, our thought processes open up, and we are more likely to approach others. We are more friendly and helpful to others when we are in a good mood than we are when we are in a bad mood, and we may think more creatively (De Dreu, Baas, & Nijstad, 2008). On the other hand, when we are in a bad mood, we are more likely to prefer to be alone rather than interact with others, we focus on the negative things around us, and our creativity suffers.
It is not unusual to feel down or low at times, particularly after a painful event such as the death of someone close to us, a disappointment at work, or an argument with a partner. We often get depressed when we are tired, and many people report being particularly sad during the winter when the days are shorter. These are normal life experiences that differ from mood, or affective, disorders. There are several types of mood disorders that are characterized into two basic categories: depression — either major depressive disorder or persistent depressive disorder — or bipolar disorder — previously known as manic-depression, of which there are three types. Mood disorders can occur at any age, and the median age of onset is 32 years (Kessler, Berglund, Demler, Jin, & Walters, 2005). Recurrence of depressive episodes is fairly common and is greatest for those who first experience depression before the age of 15 years.
Depressive Disorders
Major depressive disorder is a mental disorder characterized by an all-encompassing low mood accompanied by low self-esteem and loss of interest or pleasure in normally enjoyable activities. Those who suffer from major depressive disorder feel intense sadness, despair, and loss of interest in pursuits that once gave them pleasure (see Figure 15.12). These negative feelings profoundly limit the individual’s day-to-day functioning and ability to maintain and develop interests in life (Fairchild & Scogin, 2008). Consider the feelings of this person, who was struggling with depression and was diagnosed with major depressive disorder:
I didn’t want to face anyone; I didn’t want to talk to anyone. I didn’t really want to do anything for myself . . . I couldn’t sit down for a minute really to do anything that took deep concentration . . . It was like I had big huge weights on my legs and I was trying to swim and just kept sinking. And I’d get a little bit of air, just enough to survive and then I’d go back down again. It was just constantly, constantly just fighting, fighting, fighting, fighting, fighting. (National Institute of Mental Health, 2009, “Transcript,” para. 1, 3, 7)

According to Statistics Canada, Health Reports (Findlay, 2017), about 5% of the Canadian population suffers from major depression in a given year, with another 1.5% experiencing bipolar disorder. The highest rates are in Canadian youth aged 15 to 24, at nearly 7% (Canadian Mental Health Association, 2013). Over the course of a lifetime, approximately 13% of Canadians will meet the criteria for a mood disorder. About twice as many women as men suffer from depression (Canadian Mental Health Association, 2013). This gender difference is consistent across many countries and cannot be explained entirely by the fact that women are more likely to seek treatment for their depression. Rates of depression have been increasing, although the reasons for this increase are not known (Kessler et al., 2003). Indigenous Canadians experience depression at twice the rate of the Canadian average (Canadian Mental Health Association, 2013).
As you can see in the list below (Public Health Agency of Canada, n.d.), the experience of depression involves the mind and the body. In addition to the loss of interest, productivity, and social contact that accompanies depression, the person’s sense of hopelessness and sadness may become so severe that they consider or even succeed in committing suicide. Suicide is the leading cause of death in Canadians aged 15 to 24. In 2015, there were 4405 recorded suicides in Canada. More men commit suicide than women; however, more women are hospitalized for self-harm. Sadly, suicide is the second leading cause of death for children and youth aged 10 to 19 (Government of Canada, 2016). Depression is a significant risk factor for suicide and self-harm. Almost all the people who commit suicide have a diagnosable psychiatric disorder at the time of their death (Statistics Canada, 2019; Sudak, 2005). Indigenous Canadians have much higher rates of suicide than non-Indigenous Canadians: five times the national average for male youth, seven times the national average for First Nations women, and 11 times the national average for Inuit youth (Centre for Suicide Prevention, n.d.). Protective factors of self-government and control over local resources are associated with lower rates of suicide in some First Nations communities, all of whom are affected by the legacies of colonization, such as intergenerational trauma associated with residential school experiences and forced adoption that may increase feelings of depression and suicidal ideation.
Symptoms of depression include the following:
- Depressed mood
- Feelings of guilt, worthlessness, helplessness, or hopelessness
- Loss of interest or pleasure in usually-enjoyed activities
- Change in weight or appetite
- Sleep disturbances
- Decreased energy or fatigue without significant physical exertion
- Thoughts of death
- Poor concentration or difficulty making decisions
Bipolar disorders
Let’s consider the case of Juliana, who is a 21-year-old single woman. Over the past several years, she had been treated by a psychologist for depression, but for the past few months she had been feeling a lot better. Juliana had landed a good job in a law office and found a steady boyfriend. She told her friends and parents that she had been feeling particularly good — her energy level was high and she was confident in herself and her life. One day Juliana was feeling so good that she impulsively quit her new job and left town with her boyfriend on a road trip, but the trip didn’t turn out well because Juliana became impulsive, impatient, and easily angered. Her euphoria continued, and in one of the towns that they visited she left her boyfriend and went to a party with some strangers that she had met. She danced into the early morning and ended up having sex with several of the men. Eventually Juliana returned home to ask for money, but when her parents found out about her recent behaviour and confronted her, she acted aggressively and abusively to them, so they referred her to a social worker. Juliana was hospitalized, where she was diagnosed with bipolar disorder.
Bipolar disorders are experienced as cycles of depression and mania. Bipolar disorder is diagnosed in cases such as Juliana’s, where experiences with depression are followed by a more normal period and then a period of mania or euphoria in which the person feels particularly awake, alive, excited, and involved in everyday activities but is also impulsive, agitated, and distracted. Without treatment, it is likely that Juliana would cycle back into depression and then eventually into mania again, with the risk that she would harm herself or others in the process.
It is commonly thought that Vincent van Gogh suffered from bipolar disorder, based on his intense bursts of artistic productivity (e.g., in one two-month period in 1889 he produced 60 paintings), personal writings, and behaviour (e.g., he cut off his own ear). He committed suicide at age 37 (Thomas & Bracken, 2001). His painting, Starry Night (see Figure 15.13), offers a glimpse of the world through his eyes.
Bipolar disorder is an often chronic and lifelong condition that may begin in childhood. Although the normal pattern involves swings from high to low, in some cases the person may experience both highs and lows at the same time. Determining whether a person has bipolar disorder is difficult due to the frequent presence of comorbidity with both depression and anxiety disorders. Bipolar disorder is more likely to be diagnosed when it is initially observed at an early age, when the frequency of depressive episodes is high, and when there is a sudden onset of the symptoms (Bowden, 2001).
Although there have been important advances in research on the etiology, course, and treatment of bipolar disorder, there remains a need to understand the mechanisms that contribute to episode onset and relapse. There is compelling evidence for biological causes of bipolar disorder, which is known to be highly heritable (McGuffin, Rijsdijk, Andrew, Sham, Katz, & Cardno, 2003). However, there is much variability in the course of bipolar disorder both within a person across time and across people (Johnson, 2005). The triggers that determine how and when this genetic vulnerability is expressed are not yet understood; however, there is evidence to suggest that psychosocial triggers may play an important role (e.g., Johnson et al., 2008; Malkoff-Schwartz et al., 1998).
In addition to the genetic contribution, biological explanations of bipolar disorder have also focused on brain function. Many of the studies using functional magnetic resonance imaging (fMRI) techniques have focused on the processing of emotional stimuli based on the idea that bipolar disorder is fundamentally a disorder of emotion (American Psychiatric Association, 2000). Findings show that regions of the brain thought to be involved in emotional processing and regulation are activated differently in people with bipolar disorder relative to healthy controls (e.g., Altshuler et al., 2008; Hassel et al., 2008; Lennox, Jacob, Calder, Lupson, & Bullmore, 2004).
However, there is little consensus as to whether a particular brain region becomes more or less active in response to an emotional stimulus among people with bipolar disorder compared with healthy controls. Mixed findings are in part due to samples consisting of participants who are at various phases of illness at the time of testing (e.g., manic, depressed, or inter-episode). Sample sizes tend to be relatively small, making comparisons between subgroups difficult. Additionally, the use of a standardized stimulus (e.g., facial expression of anger) may not elicit a sufficiently strong response. Personally engaging stimuli, such as recalling a memory, may be more effective in inducing strong emotions (Isaacowitz, Gershon, Allard, & Johnson, 2013).
A series of studies show that environmental stressors, particularly severe stressors (e.g., loss of a significant relationship), can adversely impact the course of bipolar disorder. People with bipolar disorder have substantially increased risk of relapse (Ellicott, Hammen, Gitlin, Brown, & Jamison, 1990) and suffer more depressive symptoms (Johnson, Winett, Meyer, Greenhouse, & Miller, 1999) following a severe life stressor. Interestingly, positive life events can also adversely impact the course of bipolar disorder. People with bipolar disorder suffer more manic symptoms after life events involving attainment of a desired goal (Johnson et al., 2008). Such findings suggest that people with bipolar disorder may have a hypersensitivity to rewards.
Evidence from the life stress literature has also suggested that people with mood disorders may have a circadian vulnerability that renders them sensitive to stressors that disrupt their sleep or rhythms. According to social zeitgeber theory (Ehlers, Frank, & Kupfer, 1988; Frank et al., 1994), stressors that disrupt sleep, or that disrupt the daily routines that entrain the biological clock (e.g., meal times) can trigger episode relapse. Consistent with this theory, studies have shown that life events that involve a disruption in sleep and daily routines, such as overnight travel, can increase bipolar symptoms in people with bipolar disorder (Malkoff-Schwartz et al., 1998).
Explaining mood disorders
Research from family and twin studies suggests that genetic factors are involved in the development of major depressive disorder. The mode of inheritance is not fully understood, although no single genetic variation has been found to significantly increase the risk of major depressive disorder. Instead, several genetic variants and environmental factors most likely contribute to the risk for major depressive disorder (Lohoff, 2010).
One environmental stressor that has received much support in relation to major depressive disorder is stressful life events. In particular, severe stressful life events — those that have long-term consequences and involve loss of a significant relationship (e.g., divorce) or economic stability (e.g., unemployment) — are strongly related to depression (Brown & Harris, 1989; Monroe, Slavich, & Georgiades, 2009). Stressful life events are more likely to predict the first depressive episode than subsequent episodes (Lewinsohn, Allen, Seeley, & Gotlib, 1999). In contrast, minor events may play a larger role in subsequent episodes than the initial episodes (Monroe & Harkness, 2005).
Depression research has not been limited to examining reactivity to stressful life events. Much research, particularly brain imagining research using fMRI, has centred on examining neural circuitry — the interconnections that allow multiple brain regions to perceive, generate, and encode information in concert. A meta-analysis of neuroimaging studies showed that when viewing negative stimuli (e.g., a picture of an angry face or a picture of a car accident), compared with healthy control participants, participants with major depressive disorder have greater activation in brain regions involved in stress response and reduced activation of brain regions involved in positively motivated behaviours (Hamilton, Etkin, Furman, Lemus, Johnson, & Gotlib, 2012).
Other environmental factors related to increased risk for major depressive disorder include experiencing early adversity, such as childhood abuse or neglect (Widom, DuMont, & Czaja, 2007), chronic stress (e.g., poverty), and interpersonal factors. For example, marital dissatisfaction predicts increases in depressive symptoms in both men and women. On the other hand, depressive symptoms also predict increases in marital dissatisfaction (Whisman & Uebelacker, 2009). Research has found that people with major depressive disorder generate some of their interpersonal stress (Hammen, 2005). People with major depressive disorder whose relatives or spouses can be described as critical and emotionally overinvolved have higher relapse rates than do those living with people who are less critical and emotionally overinvolved (Butzlaff & Hooley, 1998).
People’s attributional styles or their general ways of thinking, interpreting, and recalling information have also been examined in the etiology of major depressive disorder (Gotlib & Joormann, 2010). People with a pessimistic attributional style tend to make internal versus external, global versus specific, and stable versus unstable attributions to negative events, serving as a vulnerability to developing major depressive disorder. For example, someone who fails an exam and thinks that it was their fault (i.e., internal), that they are stupid (i.e., global), and that they will always do poorly (i.e., stable) has a pessimistic attribution style. Several influential theories of depression incorporate attributional styles (Abramson, Metalsky, & Alloy, 1989; Abramson, Seligman, & Teasdale, 1978).
Research Focus
Using molecular genetics to unravel the causes of depression
Avshalom Caspi and his colleagues (Caspi et al., 2003) used a longitudinal study to test whether genetic predispositions might lead some people, but not others, to suffer from depression as a result of environmental stress. Their research focused on a particular gene, the 5-HTT gene, which is known to be important in the production and use of the neurotransmitter serotonin. The researchers focused on this gene because serotonin is known to be important in depression and because selective serotonin reuptake inhibitors (SSRIs) have been shown to be effective in treating depression.
People who experience stressful life events — for instance, involving threat, loss, humiliation, or defeat — are likely to experience depression, but biological-situational models suggest that a person’s sensitivity to stressful events depends on their genetic makeup. The researchers therefore expected that people with one type of genetic pattern would show depression following stress to a greater extent than people with a different type of genetic pattern.
The research included a sample of 1,037 adults from Dunedin, New Zealand. Genetic analysis on the basis of DNA samples allowed the researchers to divide the sample into two groups on the basis of the characteristics of their 5-HTT gene. One group had a short version, or allele, of the gene, whereas the other group did not have the short allele of the gene.
The participants also completed a measure where they indicated the number and severity of stressful life events that they had experienced over the past five years. The events included employment, financial, housing, health, and relationship stressors. The dependent measure in the study was the level of depression reported by the participant, as assessed using a structured interview test (Robins, Cottler, Bucholtz, & Compton, 1995).
As the number of stressful experiences the participants reported increased from 0 to 4, depression also significantly increased for the participants with the short version of the gene (see the top panel of Figure 15.14). However, for the participants who did not have a short allele, increasing stress did not increase depression (see the bottom panel of Figure 15.14). Furthermore, for the participants who experienced four stressors over the past five years, 33% of the participants who carried the short version of the gene became depressed, whereas only 17% of participants who did not have the short version did.
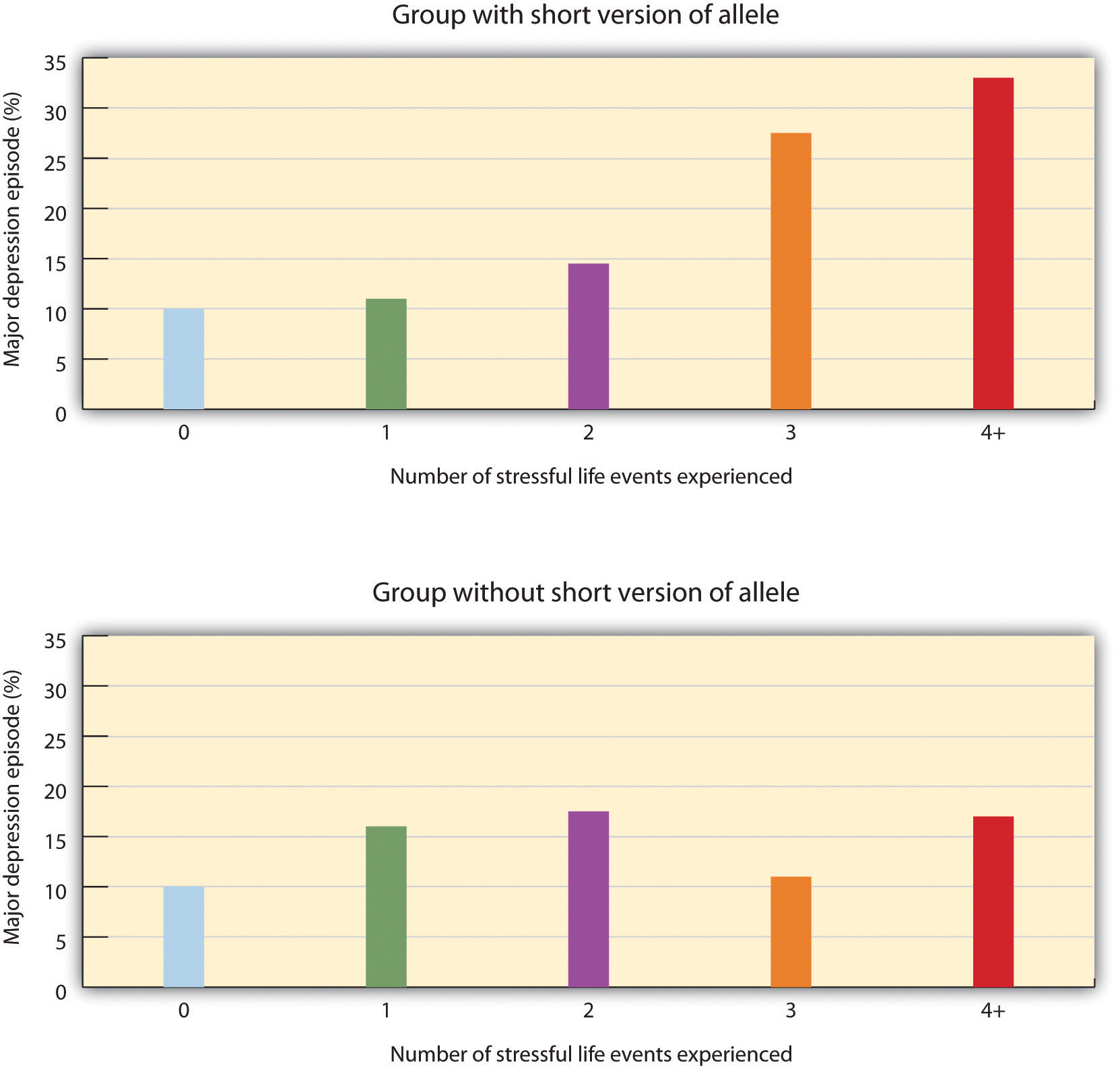
This important study provides an excellent example of how genes and environment work together. As per the findings, an individual’s response to environmental stress was influenced by their genetic makeup.
However, psychological and social determinants are also important in creating mood disorders and depression. In terms of psychological characteristics, mood states are influenced in large part by our cognitions. Negative thoughts about ourselves and our relationships to others create negative moods, and a goal of cognitive therapy for mood disorders is to attempt to change people’s cognitions to be more positive. Negative moods also create negative behaviours toward others, such as acting sad, slouching, and avoiding others, which may lead those others to respond negatively to the person — for instance, by isolating that person, which then creates even more depression (see Figure 15.15). You can see how it might become difficult for people to break out of this “cycle of depression.”

Myrna Weissman and colleagues (Weissman et al., 1996) found that rates of depression varied greatly among countries, with the highest rates in European and North American countries and the lowest rates in Asian countries. These differences seem to be due to discrepancies between individual feelings and cultural expectations about what one should feel. People from European and North American cultures report that it is important to experience emotions such as happiness and excitement, whereas people from Asian cultures report that it is more important to be stable and calm. Because North Americans may feel that they are not happy or excited but that they are supposed to be, this may increase their depression (Tsai, Knutson, & Fung, 2006).
Source: Adapted from Gershon and Thompson (2020).
Key Takeaways
- Mood is the positive or negative feelings that are in the background of our everyday experiences.
- Major depressive disorder is characterized by extreme feelings of sadness and hopelessness, coupled with other behavioural symptoms.
- Bipolar disorder is characterized by swings in mood from mania to sadness and hopelessness, and back again, with periods of near-normal moods in between.
- Mood disorders are caused by the interplay among biological, psychological, and social variables.
- Mood disorders are significant risk factors for suicide.
Exercises and Critical Thinking
- Give a specific example of the negative cognitions, behaviours, and responses of others that might contribute to a cycle of depression.
- Given the discussion about the causes of negative moods and depression, what might people do to try to feel better on days that they are experiencing negative moods?
- Why might overnight travel constitute a potential risk for a person with bipolar disorder?
- What are some reasons positive life events may precede the occurrence of manic episode?
Image Attributions
Figure 15.12. Sad Looking Woman by Bradley Gordon is used under a CC BY 2.0 license.
Figure 15.13. Starry Night by Vincent van Gogh is in the public domain.
Figure 15.14. Used under a CC BY-NC-SA 4.0 license.
Figure 15.15. Used under a CC BY-NC-SA 4.0 license.
Long Description
Figure 15.14. Genetics and causes of depression:
| Number of stressful life events experienced | Major Depression Episode (%) | |
|---|---|---|
| Group with short version of allele | Group without short version of allele | |
| 0 | 10% | 10% |
| 1 | 11% | 16% |
| 2 | 14% | 18% |
| 3 | 28% | 11% |
| 4 or more | 33% | 18% |
References
Abramson, L. Y., Metalsky, G. I., & Alloy, L. B. (1989). Hopelessness depression: A theory-based subtype of depression. Psychological Review, 96, 358–373.
Abramson, L. Y, Seligman, M. E. P., & Teasdale, J. (1978). Learned helplessness in humans: Critique and reformulation. Journal of Abnormal Psychology, 87, 49–74.
Altshuler, L., Bookheimer, S., Townsend, J., Proenza, M. A., Sabb, F., Mintz, J., & Cohen, M. S. (2008). Regional brain changes in bipolar I depression: A functional magnetic resonance imaging study. Bipolar Disorders, 10, 708–717.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington, DC: Author.
Bowden, C. L. (2001). Strategies to reduce misdiagnosis of bipolar depression. Psychiatric Services, 52(1), 51–55.
Brown, G. W., & Harris, T. O. (1989). Life events and illness. New York, NY: Guilford Press.
Butzlaff, R. L., & Hooley, J. M. (1998). Expressed emotion and psychiatric relapse: A meta-analysis. Archives of General Psychiatry, 55, 547–552.
Canadian Mental Health Association. (2013). Depression. Retrieved from https://cmha.bc.ca/documents/depression-2
Caspi, A., Sugden, K., Moffitt, T. E., Taylor, A., Craig, I. W., Harrington, H., . . . Poulton, R. (2003). Influence of life stress on depression: Moderation by a polymorphism in the 5-HTT gene. Science, 301(5631), 386–389.
Centre for Suicide Prevention. (n.d.). Indigenous suicide prevention. Retrieved from https://www.suicideinfo.ca/resource/indigenous-suicide-prevention
De Dreu, C. K. W., Baas, M., & Nijstad, B. A. (2008). Hedonic tone and activation level in the mood-creativity link: Toward a dual pathway to creativity model. Journal of Personality and Social Psychology, 94(5), 739–756.
Ehlers, C. L., Frank, E., & Kupfer, D. J. (1988). Social zeitgebers and biological rhythms: A unified approach to understanding the etiology of depression. Archives of General Psychiatry, 45, 948–952.
Ellicott, A., Hammen, C., Gitlin, M., Brown, G., & Jamison, K. (1990). Life events and the course of bipolar disorder. American Journal of Psychiatry, 147, 1194–1198.
Fairchild, K., & Scogin, F. (2008). Assessment and treatment of depression. In K. Laidlow & B. G. Knight (Eds.), Handbook of emotional disorders in later life: Assessment and treatment (pp. 213–231). New York, NY: Oxford University Press.
Findlay, L. (2017). Depression and suicidal ideation among Canadians aged 15 to 24. Statistics Canada, Health Reports 28(1), 3–11.
Frank, E., Kupfer, D. J., Ehlers, C. L., Monk, T. H., Cornes, C., Carter, S., & Frankel, D. (1994). Interpersonal and social rhythm therapy for bipolar disorder: Integrating interpersonal and behavioral approaches. The Behavioral Therapist, 17, 143–149.
Gershon, A., & Thompson, R. (2020). Mood disorders. In R. Biswas-Diener & E. Diener (Eds.), Noba textbook series: Psychology. Champaign, IL: DEF. Retrieved from http://noba.to/aqy9rsxe
Gotlib, I. H., & Joormann, J. (2010). Cognition and depression: Current status and future directions. Annual Review of Clinical Psychology, 6, 285–312.
Government of Canada. (2016). Suicide in Canada. Retrieved from https://www.canada.ca/en/public-health/services/publications/healthy-living/suicide-canada-infographic.html
Hamilton, J. P., Etkin, A., Furman, D. F., Lemus, M. G., Johnson, R. F., & Gotlib, I. H. (2012). Functional neuroimaging of major depressive disorder: A meta-analysis and new integration of baseline activation and neural response data. American Journal of Psychiatry, 169, 693–703.
Hammen, C. (2005). Stress and depression. Annual Review of Clinical Psychology, 1, 293–319.
Hassel, S., Almeida, J. R., Kerr, N., Nau, S., Ladouceur, C. D., Fissell, K., . . . Phillips, M. L. (2008). Elevated striatal and decreased dorsolateral prefrontal cortical activity in response to emotional stimuli in euthymic bipolar disorder: No associations with psychotropic medication load. Bipolar Disorders, 10(8), 916–927.
Isaacowitz, D. M., Gershon, A., Allard, E. S., & Johnson, S. L. (2013). Emotion in aging and bipolar disorder: Similarities, differences, and lessons for further research. Emotion Review, 5(3), 312–320.
Isen, A. M. (2003). Positive affect as a source of human strength. In J. Aspinall (Ed.), A psychology of human strengths: Fundamental questions and future directions for a positive psychology (pp. 179–195). Washington, DC: American Psychological Association.
Johnson, S. L. (2005). Mania and dysregulation in goal pursuit: A review. Clinical Psychology Review, 25, 241–262.
Johnson, S. L., Cueller, A. K., Ruggero, C., Winett-Perlman, C., Goodnick, P., White, R., & Miller, I. (2008). Life events as predictors of mania and depression in bipolar I disorder. Journal of Abnormal Psychology, 117(2), 268–277.
Johnson, S. L., Winett, C. A., Meyer, B., Greenhouse, W. J., & Miller, I. (1999). Social support and the course of bipolar disorder. Journal of Abnormal Psychology, 108, 558–566.
Kessler, R. C., Berglund, P. A., Demler, O., Jin, R., Koretz, D., Merikangas, K. R., . . . Wang, P. S. (2003). The epidemiology of major depressive disorder: Results from the National Comorbidity Survey Replication (NCS-R). Journal of the American Medical Association, 289(23), 3095–3105.
Kessler, R. C., Berglund, P. A., Demler, O., Jin, R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication (NCS-R). Archives of General Psychiatry, 62(6), 593–602.
Lennox, B. R., Jacob, R., Calder, A. J., Lupson, V., & Bullmore, E. T. (2004). Behavioural and neurocognitive responses to sad facial affect are attenuated in patients with mania. Psychological Medicine, 34, 795–802.
Lewinsohn, P. M., Allen, N. B., Seeley, J. R., & Gotlib, I. H. (1999). First onset versus recurrence of depression: Differential processes of psychosocial risk. Journal of Abnormal Psychology, 108, 483–489.
Lohoff, F. W. (2010). Overview of genetics of major depressive disorder. Current Psychiatry Reports, 12, 539–546.
Malkoff-Schwartz, S., Frank, E., Anderson, B. P., Sherrill, J. T., Siegel, L., Patterson, D., & Kupfer, D. J. (1998). Stressful life events and social rhythm disruption in the onset of manic and depressive bipolar episodes: A preliminary investigation. Archives of General Psychiatry, 55(8), 702–707.
McGuffin, P., Rijsdijk, F., Andrew, M., Sham, P., Katz, R., & Cardno, A. (2003). The heritability of bipolar affective disorder and the genetic relationship to unipolar depression. Archives of General Psychiatry, 60, 497–502.
Monroe, S. M., & Harkness, K. L. (2005). Life stress, the “Kindling” hypothesis, and the recurrence of depression: Considerations from a life stress perspective. Psychological Review, 112, 417–445.
Monroe, S. M., Slavich, G. M., & Georgiades, K. (2009). The social environment and life stress in depression. In I. H. Gotlib & C. L. Hammen (Eds.), Handbook of depression (2nd ed., pp. 340–360). New York, NY: Guilford Press.
National Institute of Mental Health. (2009). People with depression discuss their illness. Retrieved from http://www.nimh.nih.gov/media/video/health/depression.shtml
Public Health Agency of Canada. (n.d.). What is depression? Retrieved from https://www.canada.ca/en/public-health/services/chronic-diseases/mental-illness/what-depression.html
Robins, L. N., Cottler, L., Bucholtz, K., & Compton, W. (1995). Diagnostic interview schedule for DSM-1V. St. Louis, MO: Washington University.
Statistics Canada. (2019). Deaths and age-specific mortality rates, by selected grouped causes (Table 13-10-0392-01). Retrieved from https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310039201
Sudak, H. S. (2005). Suicide. In B. J. Sadock & V. A. Sadock (Eds.), Comprehensive textbook of psychiatry (Vol. 2, 8th ed., pp. 2442–2453). Philadelphia, PA: Lippincott Williams & Wilkins.
Thomas, P., & Bracken, P. (2001). Vincent’s bandage: The art of selling a drug for bipolar disorder. British Medical Journal, 323, 1434.
Tsai, J. L., Knutson, B., & Fung, H. H. (2006). Cultural variation in affect valuation. Journal of Personality and Social Psychology, 90, 288–307.
Weissman, M. M., Bland, R. C., Canino, G. J., Greenwald, S., Hwu, H-G., Joyce, P. R., & Yeh, E-K. (1996). Cross-national epidemiology of major depression and bipolar disorder. Journal of the American Medical Association, 276, 293–299.
Whisman, M. A., & Uebelacker, L. A. (2009). Prospective associations between marital discord and depressive symptoms in middle-aged and older adults. Psychology and Aging, 24, 184–189.
Widom, C. S., DuMont, K., & Czaja, S. J. (2007). A prospective investigation of major depressive disorder and comorbidity in abused and neglected children grown up. Archives of General Psychiatry, 64, 49–56.
